Schulman Blitz, LLP Settles Medical Malpractice Wrongful Death Case For $1.95 Million
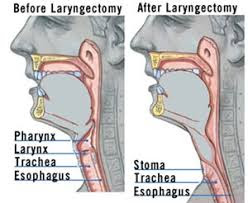
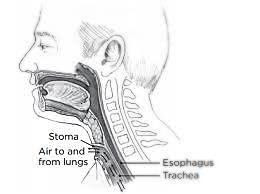
When our client Robert first came to Schulman Blitz, LLP, his potential malpractice case had already been turned down by several other top New York law firms. Robert told us that he was married, and that he had recently become a father to a young daughter. He told us that he had graduated from the University of Michigan and went on to become an acclaimed painter, writer and artist. Robert also told us that he was a survivor of cystic fibrosis, a disease he had been living with since being diagnosed as a child. In fact, by the time he first came to us, Robert had already outlived the life expectancy of an average cystic fibrosis patient. He told us that he already had a kidney transplant and two double lung transplants prior to any of the malpractice he alleged had even occurred. Robert, admittedly, did not have long to live. Additionally, the malpractice claims that he was making were against the surgeon who performed his second double lung transplant, a highly regarded physician who not only had saved his life with a successful double lung transplant surgery, but who was also one of the world’s top lung transplant surgeons as well as the director of the lung transplant program at one of the best hospitals in the country. Robert’s medical records consisted of over 30,000 pages, which we analyzed meticulously and sent to our team of experts for review. The first batch of expert physicians that we retained could not all collectively agree that malpractice had actually occurred, and they were not convinced that we had a viable case to pursue on Robert’s behalf. But we were undeterred. The second group of expert physicians that we retained to review the records all agreed that malpractice had in fact occurred and that Robert’s ongoing pain and suffering resulted from the negligent post-lung transplant care of his surgeon. We then filed a medical malpractice lawsuit on Robert’s behalf and proceeded to litigate the case. The malpractice arose during the months and years after Robert received his second double lung transplant, while he was an outpatient at the Adult Lung Transplant Program at a world–renowned New York City hospital. The program required Robert to go to the hospital periodically for his surgeon to conduct postoperative surveillance bronchoscopies, a procedure in which a camera was inserted through Robert’s mouth and down his throat, to allow his surgeon to view his lungs and determine the success of the lung transplant. It was during this time when a small granuloma was first seen on Robert’s vocal cords. Despite noting the presence of the granuloma in Robert’s medical records, nothing was done to treat it. Over the course of about a year, the small granuloma grew to a nodule and then to three nodules. Despite the fact that lung transplant recipients are at a much higher risk of developing cancer due to the immunosuppressant medications that they are required to take so that their body does not reject the new lungs, nothing was done to treat the nodules that were clearly visible through the camera that was being used during the bronchoscopies. Eventually, those nodules grew to become a lesion that developed into stage IVa cancer of the larynx and a hyper-intensive lobulated mass of his vocal cords and airway. The cancer required Robert to undergo a total laryngectomy, a surgery done to remove Robert’s voice box. Without his voice box, Robert lost his ability to speak and communicate with his wife and daughter. He was forced to write words down on paper or mouth words to communicate. Eventually, even that became too difficult, as the cancer had begun to spread to other parties of his body. Additionally, Robert lost the ability to chew solid food and required all food that he ingested to be in liquid form. In order to get proper nutrition, Robert had a percutaneous endoscopic gastrostomy (PEG) tube implanted into his stomach.
As a result of the cancer that developed from the untreated granuloma and nodules on his vocal cords, Robert had to undergo radiation treatment, chemotherapy, and placement of a tracheoesophageal prosthesis. Robert also had to use a bi-level positive airway pressure machine (BIPAP) on a daily basis. Eventually, as the cancer spread, Robert became completely immobile and was unable to ambulate without wheelchair assistance. Robert would require 24-hour nursing care for all aspects of daily life, and he underwent multiple hospital admissions due to recurrent leakages from the prosthesis that would cause aspiration pneumonia. We quickly realized that Robert would unlikely survive the duration of the lawsuit, so we arranged for a videographer to film a video documenting a typical day in his life, for the purpose of preserving the evidence of his daily suffering, should a jury need to see it in the future at a time when Robert would no longer be with us. As expected, Robert passed away during the course of litigation, due to consequences from the cancer, including septic shock, triple organ failure, recurrent renal failure and double pneumonia, all of which led to his needless death. As such, we filed an Amended Complaint against the doctor and the hospital to not only assert claims for medical malpractice, but also to allege a cause of action for wrongful death. The case was vigorously defended by one of the top medical malpractice defense law firms in New York, and the litigation continued for over fours years. Justin Blitz, Esq. conducted a three day long deposition of the defendant surgeon, among many other depositions of various witnesses. During this litigation, Schulman Blitz, LLP retained experts in otolaryngological surgery, pulmonology, lung transplantation, oncology, cystic fibrosis, and economics to prove our case on behalf of our client, who was now Robert’s widow. With the help of our experts, and through Mr. Blitz‘s tireless efforts, we were able to show that as a result of the malpractice, Robert endured tremendous pain and suffering and had to undergo many medical procedures, which further exacerbated his pain and suffering. After the defendants’ motion to dismiss our case was vigorously opposed and then denied by the court, and after over five years of litigation, we agreed to an out of court mediation. We prepared a video that was played during the mediation, which documented Robert’s life, the malpractice, terrible suffering, and Robert’s eventual death that occurred as a result of the surgeon’s negligence. Justin Blitz, Esq. and Fred Schulman, Esq. settled Robert’s case at mediation for $1,950,000, an amount that will provide for his widow and his daughter for years to come.
Justin Blitz and I have been friends for many years. I give him and his firm the highest review possible.Justin told me, "if i can ever be of help to you don't hesitate to call me".I have referred cases of friends and family members to Justin for his help and he always responded in a prompt and professional manner. He has a great deal of experience in the New York Court System and a vast knowledge of the law.There are many lawyers in New York City, Justin is one of the best and more importantly, Justin is a lawyer I can trust.
I’m very grateful for the Schulman Blitz law firm. They took my case and handled it in a very responsible way. I couldn’t be more happy with the end results. They addressed all my concerns and I was always treated with respect. Again I’m very grateful for the whole Schulman Blitz team. God bless you all. You are a wonderful law firm
Best law firm in New York. They made me feel supported throughout the entire case. They addressed all of my questions and concerns promptly. They kept me informed of the progress of my case. They make you feel and show with their actions that they have your best interest at heart. I am extremely happy with the outcome of my case. I highly recommend Schulman Blitz to anyone who is looking for a law firm, which will fight for your rights and will do its utmost to get you the maximum compensation that you deserve. Forget the rest, Schulman Blitz is the best!
Fred and Justin were there for me from the very beginning to the end. They made sure that I had no worries while I was recovering from my injuries and helped me along the way. Every question that I asked was answered truthfully. They made me feel like family and even after my settlement they have kept in contact with me. I have even referred Fred and Justin to a few friends that had positive results in their cases. These guys make you feel like family because they treat you like family. Schulman Blitz are the best lawyers in town because of their professional understanding and good value and how they make their clients feel comfortable knowing that they are in good hands.
I absolutely love Schulman Blitz! This firm is wonderful and prides it’s self on professionalism. I’ve had the pleasure of working with various people from this firm (Justin Blitz, Thomas etc.) and they take care of everything and never leave you second guessing! Also their communication is impeccable and as you’ll see the most work you’ll have to do is to pick up your phone and they’ll handle the rest! Outstanding team of people! New York’s best kept secret! C.I
Blitz Law Group, LLP, renowned for handling personal injury cases throughout the entire state of New York, is thrilled to announce the successful resolution of a deeply tragic case. Our client, a 38-year-old man, tragically lost his life after being improperly discharged from an upstate New York, Albany area hospital. He leaves behind his loving wife and three young children.
Blitz Law Group, LLP is pleased to announce the successful settlement of our client’s case for $3.75 million. This case centered around the medical treatment received by a cherished member of the Far Rockaway community known for his vibrant personality and numerous talents.